Causative & risk factors
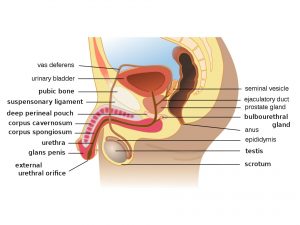
Male hypogonadism can be classified into primary and secondary. In primary hypogonadism the problem lies in the testes whereas in secondary hypogonadism the problem lies in the hypothalamus or the pituitary gland.
The causes of primary hypogonadism include undescended testicles, testicular injury, mumps orchitis, primary hypogonadism, Klinefelter syndrome and hemochromatosis. Radiation therapy or chemotherapy are also known causes of primary hypogonadism.
Secondary hypogonadism can result from any condition that impairs the functioning of the hypothalamus or the pituitary gland. These include surgery or radiation therapy in the brain tissue, diseases like tumors, tuberculosis, HIV or sarcoidosis affecting the brain tissue and Kallmann syndrome. Advancing age and obesity are known risk factors. Excessive physical or emotional stress can also cause a temporary deficiency of testosterone.
Clinical presentation
Hypogonadism can begin at any age ranging from fetal life to adult life.
If this condition begins in fetal life, the external male sex organs may be underdeveloped. In their place, the child may develop female or ambiguous genitals.
When hypogonadism begins at puberty, the child may lack in typical male characteristics and may have lack of body hair, a low muscle mass and inadequate growth of the testes and the penis. In addition his voice may not be deep enough and he may develop excessive breast tissue (gynecomastia).
When hypogonadism begins in adult males, their existing muscle mass and body hair growth may reduce. He may also develop erectile dysfunction and infertility. He may develop osteoporosis and gynecimastia.
Reduced testosterone levels gives rise to symptoms like low libido, weakness and even hot flashes.
Investigations
After a thorough medical history and physical examination, the blood testosterone levels are tested. Semen analysis and a testicular biopsy may be performed. This may be followed up with brain imaging studies and genetic testing.
Treatment
For younger children the treatment mainly consists of testosterone replacement therapy along with the use of pituitary hormones if necessary. Testosterone can be administered in the form of injections, application of a patch or gels. Other delivery methods include implanting testosterone pellets under the skin or through the buccal cavity.
Treatment for adults also consists of testosterone replacement therapy and pituitary hormones if necessary. In addition to this if the pan make use of assisted reproductive techniques.