Causative & risk factors
Morphea is thought to be an immune-mediated disorder. The exact mechanism is not known. It can be triggered by certain infections, exposure to radiation and repetitive trauma to the specific location.
Clinical presentation
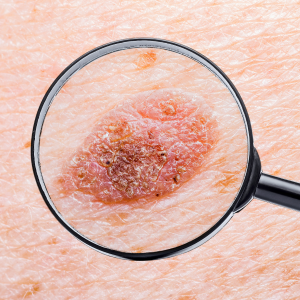
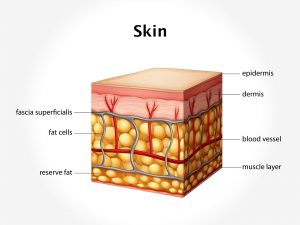
The skin in the affected area becomes thick, hard and discolored. The area becomes covered with discolored patches. These patches eventually become centrally white. The affected area becomes devoid of hair and sweat glands.
Depending upon the number and location of the skin lesions, morphea can be classified into various types such as:
Circumscribed – The commonest form of morphea, presenting with less than 3 lesions.
Generalized – 4 or more lesions, affecting 2 or more regions of the body.
Superficial – Characterized by purplish patches in the folds of skin of middle-aged women.
Linear – Linear presentation of lesions, commonly seen in children.
Pansclerotic – A severe form of the disease, affecting children, leading to the formation of contractures, non-healing ulcers and squampos cell carcinoma.
Investigations
Morphea can be diagnosed on the basis of the appearance of the skin. A skin biopsy may be done for confirmation.
Treatment
Morphea is an incurable condition. Sometimes it may get better on its own without any treatment. To reduce the symptoms, the physician may prescribe anti-malarial drugs, corticosteroids and other immune-suppressive drugs.
Topical applications containing vitamin D help to relieve the symptoms.
Ultraviolet light therapy helps reduce the skin discoloration.