Causative & risk factors
The exact cause is yet to be found out. However it is clear that pityriasis rosea is not a bacteria or fungal infection. It is probably caused by a virus, however it is not contagious.
Clinical presentation
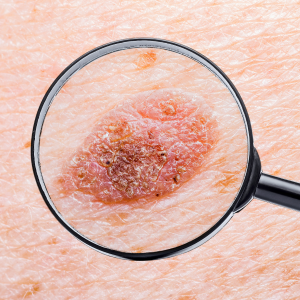
Pityriasis rosea begins with the sudden appearance of 1 primary lesion, which is red, circular and slightly elevated (mother rash). The lesion has fine scales and is centrally clear, giving it a ring-shaped appearance. Within a few days, several such ring-shaped lesions develop on the body (daughter patches).
The primary site of affection is the trunk and the proximal portions of the limbs. The lesions present on the back are arranged symmetrically along the rib lines thus giving the appearance of a ‘Christmas tree’. In severe cases, the entire arms, legs and the face may be involved.
About half the patients develop itching. Some people may develop blisters on the rash.
The appearance of the rash may be preceded by prodromal symptoms like headache, loss of appetite, nausea etc.
Investigations
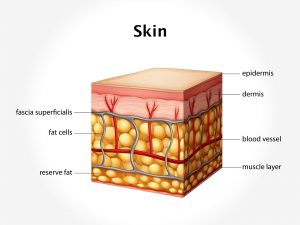
Pityriasis rosea can be diagnosed on the basis of clinical examination of the lesions by a physician. A potassium hydroxide skin test is performed to rule out fungal infections. In case of doubt, a skin biopsy may be performed.
Treatment
Even without treatment, the condition resolves on its own within 4 to 6 weeks.
The use of soaps or any irritating substances on the skin must be avoided. Soothing lotions may be suggested for relieving itching, if present.
Topical steroid creams may be prescribed to some patients. Antiviral drugs when prescribed at the onset of the illness help to cut short the course of illness.
Most patients will never have a recurrence of pityriasis rosea.