Causes and risk factors
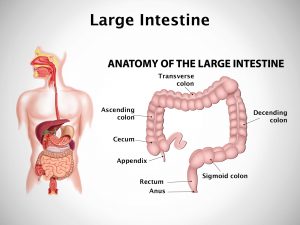
Pneumatosis cystoides intestinalis occurs as a complication of connective tissue disease like scleroderma with multiple gas-filled cysts which are found in submucosal or subserosal layer of intestinal wall, especially terminal ileum. When the cysts rupture, they cause pneumoperitoneum. Intestinal involvement in diseases like systemic sclerosis, polymyositis, dermatomyositis, or mixed connective tissue disease may be complicated by PCI. Various theories have been put forth for the pathogenesis of PCI. One theory says the mucosal breakdown due to steroids and similar immunosuppressive agents can cause shrinkage of Peyer’s patches in the intestine which can lead to the condition. Bacterial theory says that fermentation of carbohydrates by bacteria can lead to excess gas formation in the intestine causing its absorption in the wall of intestine. Disease associated with PCI include COPD, connective tissue disorder, infectious enteritis, and celiac disease.
Clinical presentation
Many a times the patient is asymptomatic. Patient presents with pain in abdomen with distension. Pain is crampy and diffuse. Fever may be accompanied with pain. Abdominal tenderness is present. Patient complains of chronic constipation. There may be diarrhea. Patient suffers from blood loss from rectum. There may be history of chronic obstructive pulmonary disease and finger clubbing.
Investigation
Medical history by the patient and clinical examination by the doctor can help in diagnosis. Routine hemogram is done. Abdominal plain x-ray is advised. Endoscopy is recommended. Colonoscopy is required. Imaging studies such as CT scan of abdomen may be useful for further evaluation. Tissue biopsy is done which confirms the diagnosis.
Treatment
Treatment depends upon the underlying cause. Treatment of underlying systemic disease should be done. Symptomatic treatment with analgesics and antipyretics is given. First line of treatment in severe cases is oxygen therapy. It involves increasing partial pressure of oxygen in the blood, which in turn increases pressure gradient of gas in the cyst. The cysts release gas present within them and refill with oxygen, which is then metabolized. Further treatment consists of surgical intervention such as laparotomy.