Causes and risk factors
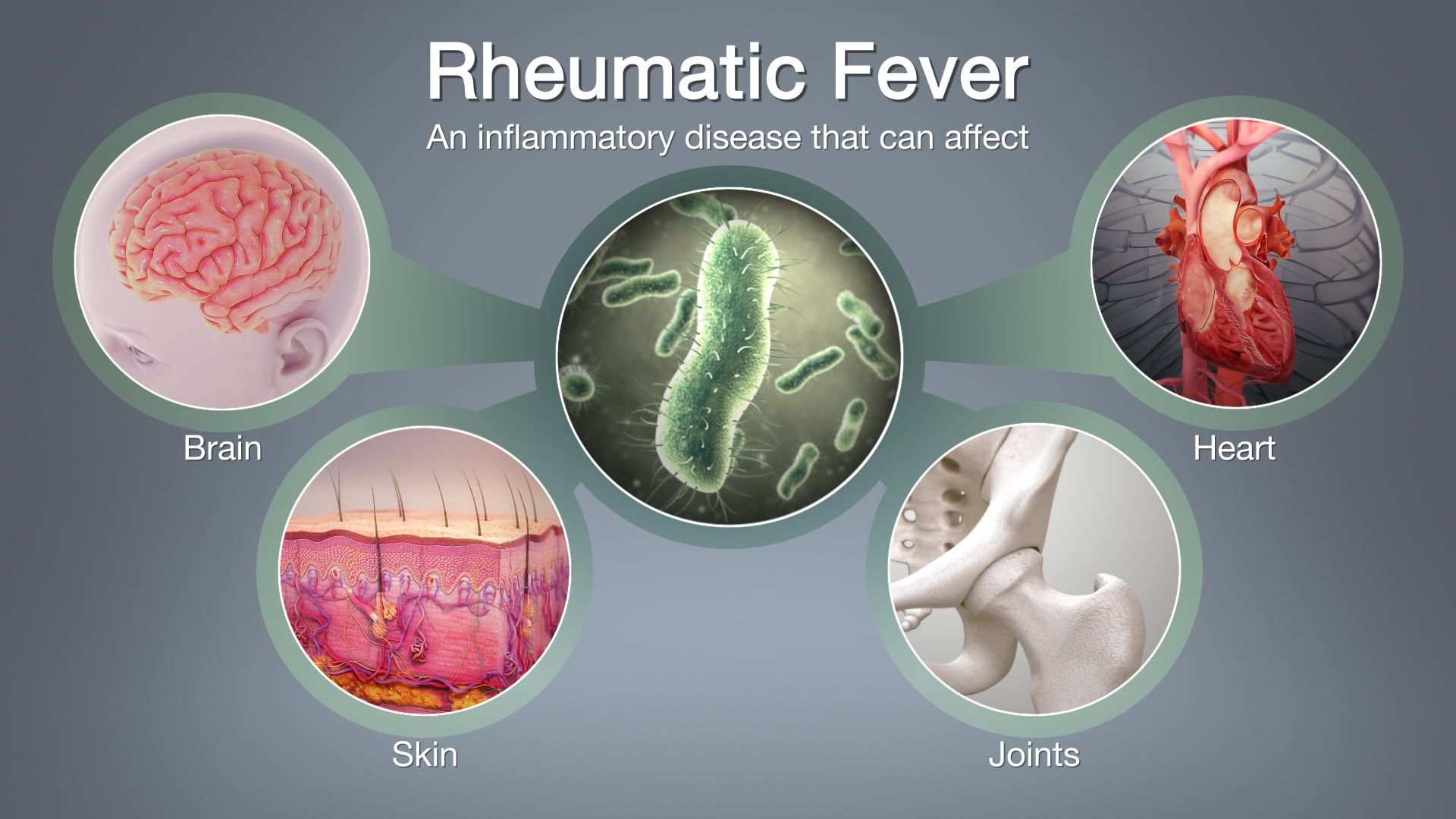
The cause of rheumatic fever is a defective immune reaction. The body gives a delayed immune response to infection with certain organisms known as group A streptococci. This in turn leads to inflammation in various body structures.
Primarily the heart is affected. Additionally skin and joints are also affected.
The risk factors for development of rheumatic fever include overcrowding and poor hygiene practices. Hence rheumatic fever occurs commonly in low socio-economic groups.
Clinical presentation
History of sore throat is usually present about 2 to 3 weeks prior to development of symptom of rheumatic fever. Arthritis and arthralgia of large joints occurs. Symptoms of carditis (inflammation of the heart) and Sydenham’s chorea (muscular weakness and involuntary muscular movements) appear. Skin rashes are seen in the form of red blotches. Subcutaneous nodules may be observed on the bones or tendons.
Complications such as damage to the heart muscles or valve and cardiac failure may arise.
Diagnosis & Investigations
A complete blood count will demonstrate leucocytosis. The ESR and CRP will be raised. Throat swabs and ASO titres (antistreptolysin antibodies) may be recommended to confirm streptococcal infection. An electrocardiogram and a chest X-ray are performed. An echocardiogram may reveal mitral prolapsed or mitral regurgitation.
‘Jones criteria’ have been laid down to make a diagnosis of rheumatic fever. Rheumatic fever can be diagnosed if 2 or more major criteria are fulfilled or if 1 major and 2 or more minor criteria are fulfilled.
The major criteria include:
- Carditis
- Polyarthritis
- Chorea
- Erythema marginatum
- Subcutaneous nodules
The minor criteria include:
- Fever
- Arthralgia
- Previous rheumatic fever
- Raised ESR (erythrocyte sedimentation rate) or CRP (C reactive protein)
- Arthralgia
- Previous rheumatic fever
- Raised ESR or CRP
- Leucocytosis
- First degree AV block
Treatment
Bed rest is essential until recovery takes place. Penicillin is the drug of choice. It may be given orally or in injectible form. Antibiotics may be continued on a long term basis (several years) to prevent recurrence. Other drugs frequently used are aspirin and corticosteroids.
The following steps can be taken to reduce the incidence of rheumatic fever:
- Better sanitation will help to bring down the instances of rheumatic fever.
- All children with strep throat or scarlet fever must be adequately treated. One must ensure that they are completely free of infection once the medications are over.
It is necessary to administer long term antibiotics to prevent a second attack of rheumatic fever.