Causative & risk factors
Scoliosis can be congenital, idiopathic, neuromuscular or degenerative. Congenital scoliosis is present in infants since birth. Idiopathic scoliosis occurs in adolescents, with no underlying cause. Neuromuscular scoliosis occurs as a result of musculoskeletal abnormalities such as spina bifida. Degenerative scoliosis occurs as a result of injury, surgery, osteoporosis or other bone disorders.
Scoliosis can run in families. Females have a slightly higher risk of developing scoliosis.
Clinical presentation
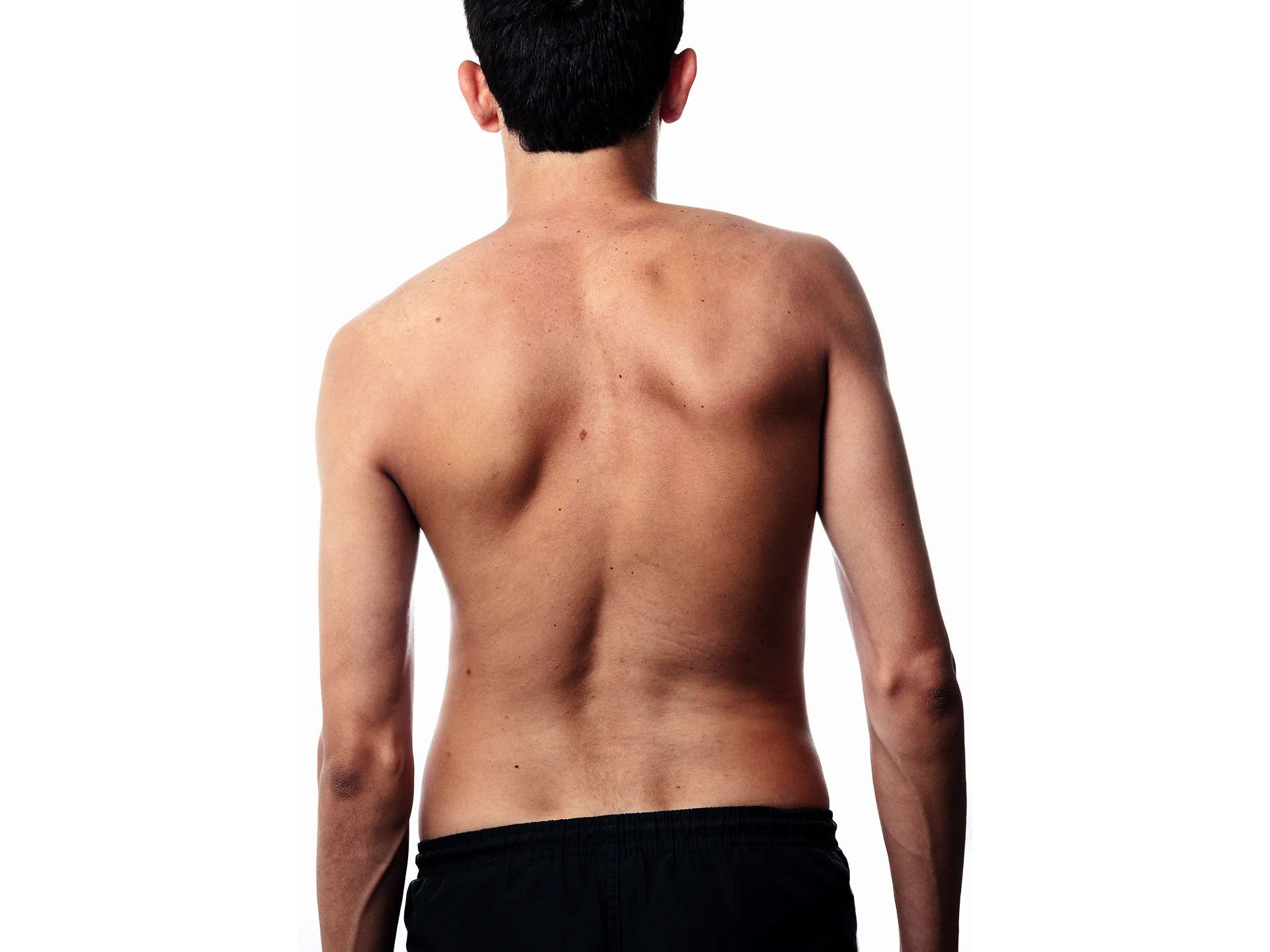
Depending upon the degree of scoliosis, the spine will appear curved. The shoulders may appear uneven. The waistline may not appear symmetrical with 1 hip positioned higher than the other. Severe scoliosis can give rise to back pain.
Investigations
Physical examination of the spine involves visual inspection of the spine as well as certain physical tests like kneel-down and bend down. An X-ray is done to confirm the diagnosis of scoliosis. Occasionally an MRI, CT or bone scan may be advised.
Treatment
Mild scoliosis less than 20 degrees needs only to be monitored. A higher degree of scoliosis in adolescents is treated with back braces in order to avoid further progression of the curve.
People with severe scoliosis, more than 40 degrees are offered surgery. Surgery involves use of metallic structures to hold the spine in place and placement of bone grafts. The ultimate result is a fusion of the spinal vertebrae. This surgery is only done on patients who have attained complete bone growth.
Recent updates
Genetic testing has been developed which can help detect whether a child with scoliosis will have mild, moderate o severe progression of scoliosis in the future.